The UK Public Sector Digital User Needs Revolution
The GDS has set out a series of very clear design principles to facilitate the transition to a Digital by Default Government and a Social Economy. These start with end user needs and mandate that the ensuing services fit those needs. This is in preference to making the intended user conform to poor system design, often across
multiple service providers (for example, different and unconnected Government Departments of State, as has been the historic model.
In effect, this focus on true user needs at the interface with computer systems represents the next revolution in digital transformation. It is a revolution which clinicians at the NHS coal face and beyond would do well to study and understand, not least through the regular and highly informative Blog postings of the GDS,.
Buoyed by the theoretical benefits of the Digital Economy, the UK Department of Health has mandated a total transition from a paper based economy to a wholly digital health economy before the end of this decade.
Regrettably, this transition has not been backed by any significant or meaningful investment in end user research for clinicians at the digital and clinical coal face, whether in Primary Care or in Hospital Practice. Moreover, given the adverse coverage on the huge investments in NHS IT, and given the apparent failure of top down direction of health service informatics and centralised decision making, the Department of Health has effectively devolved IT decision making and systems acquisition to individual Trusts.
Thus, at the very moment at which GDS principles are coming of age across the UK Public Sector IT Estate, Health has detached itself from the Change Process at local level in favour of local solutions and individual commercial arrangements.
Digital by Default Design for Surgeons
Surgeons across the country will have very different experiences of Informatics, depending upon which IT route the individual NHS Trusts have chosen to travel, and which systems the management teams have chosen to purchase. In general terms, experiences will be nevertheless suboptimal, with clinical staff using systems:
- which have rarely if ever been properly tested, adapted and optimised other than in the most cursory fashion for the practical end user needs of clinician and allied health professionals:
- and which have been acquired primarily for managerial and administrative functions.
It is probably fair to observe that in most cases, the uptake of digital systems by clinicians has been through compulsion rather than through volition, and that the vast majority of integrated Electronic Patient Record (EPR) systems at Trust level are significantly suboptimal in daily use. There are nevertheless bright spots, such as the national PACS system.
My own Trust in Southampton has been at the forefront of IT innovation since the mid 1990s. It has a large, complex and data rich digital estate. Digitally aware clinicians engage in a continuous collaborative discussion with our IT managerial colleagues as to how best to identify and address the continuing shortcomings in our existing systems, particularly in relation to the quality of the clinician-facing interfaces.
The Scourge of the PDF Document
A key element in this debate has been the recognition of the need to move on from systems that merely “do things”, such as move documents, reports and images around the hospital’s virtual IT estate. In the process of moving from paper to electronic clinical records, the initial solution has been simply to capture hand-written documents and reports in PDF format, and then to present them to the clinician in a busy clinic in list mode.
Unfortunately, all of us with any experience of such methodology can testify as to how slow and debilitating the trawl through PDF documents can be as a means of accessing key clinical information, when compared with speed reading traditional paper record folders.
This “first generation paperless” methodology has substantial and generally hidden productivity costs which have yet to be widely recognised. In my own clinical service, we found that we needed to drop five outpatient slots per clinic to accommodate the time spent on looking up and cross referencing electronic documents as compared to traditional methods. This prompted rapid administrative recognition of the challenges of digital change.
This observation has led to the adoption and testing of novel IT tools for data presentation and visualisation such as the University Hospital Southampton (UHS) Lifelines EPR visualisation system (Fig 1); and the rigorous classification of all further documents using metadata to define their contextual relevance in daily use. This is both through in house design and through discussion with our preferred commercial suppliers.
The ASGBI and the Digitally Educated Surgeon
It is clear that there is much work to be done to make best use of the digital transformation of clinical information, and that excellence in this process will produce substantial efficiency gains for the NHS. The specific design needs of the clinician end user have been largely neglected to date, resulting in time loss and frustration within the “Digital Compulsion” environment within which most of us work.
It is therefore necessary for surgeons to understand the possibilities of excellent, user focussed design in the efficient delivery of public sector health care; and to engage with management colleagues and information specialists at all levels in the Health Service in the development of better systems than are presently on offer. Success in this radical evolutionary process could and should lead to a transformation in service delivery across health and social care in the UK and beyond. Failure in design and implementation will lead to needless costs and greater inefficiencies, as the laws of unintended consequences are once again enacted across the NHS IT estate.
The ASGBI will continue to play a significant role in the education of surgeons in this complex subject area (3), and to build on the achievements of the theme of the Digital Surgeon of the 2016 Belfast Conference, where we were delighted to run both a plenary session on Clinical Informatics, and a symposium on Health Technology in partnership with the Engineering and Physical Sciences Research Council, about which there are other articles in this issue. We encourage all with experience, knowledge and insights in the subject area to contribute to the educational process through articles for future editions of the Journal.
References
- UK Government Digital Service Design Principles: https://www.gov.uk/design-principles
- A strategy for Digital Public Services in New Zealand: Search www.ict.gov.nz
- Rew DA. The Clinical Informatics Revolution. An Issue in Professional Practice of the ASGBI. http://www.publications.asgbi.org/ciiipp_04_15/clinical_informatics_ipp.html
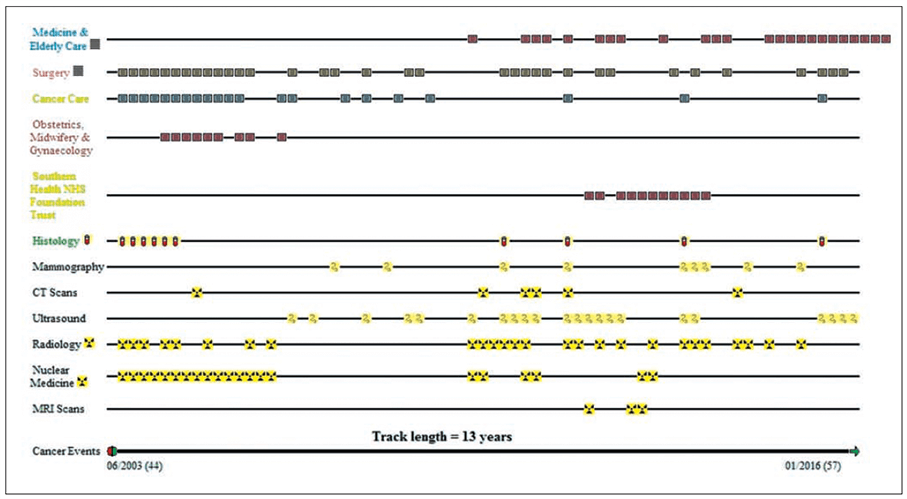
Figure 1: The UHS Lifelines graphical EPR interface, as an illustration of user focussed design in the paperless transition. This system is in live and real time daily use on an agile, continuously iterative test and development basis in selected clinical services at University Southampton. This particular record illustrates the documents generated in the course of treatment of a patient with bilateral breast cancer in June 2003. Clicking on any document opens the underlying document. All subject timelines (eg Surgery, Cancer Care) for which documents exist are displayed. It is apparent how quick and intuitive such a model can be in clinical use. Much can be learned about the pattern of health in any one patient from inspection of the patterns of documentation alone, before inspection of specific documents and reports.
JOIN US FOR THE 10th ANNUAL ACPGBI MEETING
Bournemouth × 3–5 July 2017
KEYNOTE AND SYMPOSIA TOPICS INCLUDE:
- Lars Påhlman Memorial Lecture
- War, austere environment and natural disaster surgery
- What’s new in the world of research?
- International Trial / guideline updates
- Adolescent colorectal disease
- Lessons learned and shared
- “My worst day” - when things go wrong
- BJS lecture SPECG
- IBD reconstructive surgery
- International Nursing Congress
- Controversy debates in colorectal disease
- Peri-operative management
- Managing the obese patient with colorectal disease
- Living with colorectal disease
- Video abstract sessions
- 1st EBSQ Exam in UK
- Cycle charity ride in aid of BDRF
- Golf
- 4th July Celebration Gala Event
- Charity / Patient day session
More information is available now on the conference website - www.acpgbiconferences.org.uk
Follow us on twitter - @acpgbi #acpgbi2017

